 About Margot
About Margot
Born in 2000, Margot went straight into the NICU for a month
 GoPro Hero
GoPro Hero
Everyday, incredible
accomplishments captured on video
 Smile!
Smile!
3 providers, 4 months, 5 appointments, too many phone calls, to fix 1 cavity
 Real food, real meals
Real food, real meals
From drip-feeding a chemical blend to real food. Recipes included!
 No "Can't Do"
No "Can't Do"
A new video challenging assumptions about what Margot can enjoy and do.
 Siege or surrender
Siege or surrender
On a Christmas trip to the tropics, I waved a white flag to our new reality.
 Prisoner of Routine
Prisoner of Routine
Creating functional & fun routines took lots of effort but salvaged our sanity.
 Trail Adventures
Trail Adventures
A blog for the Rails to Trails Conservancy offers tips to help hit the trails.
 Leap of faith: Act I
Leap of faith: Act I
My hopes took a hit, so I needed inspiration to take risks again, like kayaking.
 Leap of faith: Act II
Leap of faith: Act II
Inspired to kayak? From idea to implementation, and a lesson for research.
 It's all downhill!
It's all downhill!
Can Margot learn to ski? With expert help and sensible teaching, yes!
 Best summer ever!
Best summer ever!
After 18 years, getting summer right for Margot and the whole family!
Enjoying real food and real meals
Helping Margot transition from a drip feed of Pediasure to full meals of healthy foods
Originally published November 2, 2016; Updated December 2, 2016, and January 3, 2019
 Our lives revolve around food. But what if the only food you got was a blend of chemicals that was delivered drip by drip through a pump that you were tethered to for hours every day, and that left you constipated (and therefore irritable) and underweight? That could have been Margot!
Our lives revolve around food. But what if the only food you got was a blend of chemicals that was delivered drip by drip through a pump that you were tethered to for hours every day, and that left you constipated (and therefore irritable) and underweight? That could have been Margot!
After a long journey, Margot now has four "meals" a day that consist predominantly of real food. Ironically, we have turned her her disability to her advantage: though she is still tube fed, she has the potential for a diet far healthier than most Americans (you can read more about Margot's current recipes here). She is at a healthy weight and no longer constipated. And we initiated most of the steps along the way on our own, with remarkably little guidance from professionals. So this is also a story of breakdowns in implementation that affect even the most basic care for other children like Margot. This lesson is similar to what I have observed (and sought to redress) in children on the autism spectrum with respect to (too many) other needs.
Some background
 Some children are tube-fed because their bodies cannot process food quickly and/or easily. This was not the concern for Margot: she simply could not easily coordinate her swallow, which meant that she was at risk of choking on solid food or aspirating liquids (we had been working for years on a separate oral feeding program for her - more about that another time). When Margot was an infant, she was fed a liquid formula (enteral pediasure) through a nasogastric (NG) tube, as in the picture on the left. Margot could easily pull her NG tube out (which she did often) until we replaced this with a more permanent MIC-KEY tube when she was 14 months of age. Putting an NG tube back in is one of the worst things a parent can do to their child, as the experience of prisoners force-fed at Guantanamo attests to.
Some children are tube-fed because their bodies cannot process food quickly and/or easily. This was not the concern for Margot: she simply could not easily coordinate her swallow, which meant that she was at risk of choking on solid food or aspirating liquids (we had been working for years on a separate oral feeding program for her - more about that another time). When Margot was an infant, she was fed a liquid formula (enteral pediasure) through a nasogastric (NG) tube, as in the picture on the left. Margot could easily pull her NG tube out (which she did often) until we replaced this with a more permanent MIC-KEY tube when she was 14 months of age. Putting an NG tube back in is one of the worst things a parent can do to their child, as the experience of prisoners force-fed at Guantanamo attests to.
Moving Margot from a drip feed to a full "meal"
 When she was very young, Margot also had reflux, which sometimes led her to gag and vomit, and then sometimes choke. To control this, she was initially fed more gradually - a constant "drip" for an hour at a time, 4-5 times a day, using a Kangaroo pump. While the technology is incredible, it still means that she is hooked up to a pump 4-5 hours a day, like in the picture on the right. If she moved around, she could easily pull out her tube. I had completed a predoctoral rotation in an infant feeding program at the Montreal Children's Hospital, and so was familiar with the steps involved in moving children to more substantial feeds.
When she was very young, Margot also had reflux, which sometimes led her to gag and vomit, and then sometimes choke. To control this, she was initially fed more gradually - a constant "drip" for an hour at a time, 4-5 times a day, using a Kangaroo pump. While the technology is incredible, it still means that she is hooked up to a pump 4-5 hours a day, like in the picture on the right. If she moved around, she could easily pull out her tube. I had completed a predoctoral rotation in an infant feeding program at the Montreal Children's Hospital, and so was familiar with the steps involved in moving children to more substantial feeds.
 After several months of being tethered to a pump, no one had suggested a course of action, so I proposed a plan to Margot's physician to move her to a faster feeding schedule: she thought it was a great idea! I tracked Margot's vomiting, and began to progressively shorten the length of her feed (i.e., so that she was getting a greater quantity in a shorter period of time). Within several months, we had moved her off of the pump entirely, delivering her feed over a 5-10 minute span instead of a 60 minute span, and using large syringes instead of a pump. The picture above shows me delivering a quick "meal" at a picnic table beside a beautiful bike trail in the Lehigh Valley.
After several months of being tethered to a pump, no one had suggested a course of action, so I proposed a plan to Margot's physician to move her to a faster feeding schedule: she thought it was a great idea! I tracked Margot's vomiting, and began to progressively shorten the length of her feed (i.e., so that she was getting a greater quantity in a shorter period of time). Within several months, we had moved her off of the pump entirely, delivering her feed over a 5-10 minute span instead of a 60 minute span, and using large syringes instead of a pump. The picture above shows me delivering a quick "meal" at a picnic table beside a beautiful bike trail in the Lehigh Valley.
Fattening Margot up
As a toddler, Margot had difficulty gaining weight. During my predoctoral rotation, I had also learned of a calorie-boosting powder. No one recommended this supplement. I finally tracked down such a supplement (Duocal), which could increase the number of calories she was getting by 50%. Despite the fact that Margot was diagnosed with failure to thrive, we could not get a prescription for Duocal approved for about a year, During the interim, we bought it off of Ebay!
Pediasure: The ultimate processed food
Pediasure is the ultimate processed food, with its ingredients listed in a recent blog. If you have also read the origins of the ingredients in a Twinkie, you will learn how some of ingredients common to processed foods are manufactured or even mined. A Pubmed search only uncovers a handful of articles on the possible benefits of Pediasure (quite remarkable given the amount that is likely sold), and no articles demonstrating its superiority to the kind of blended diet described below. And this is even more remarkable given how profitable Pediasure and other formulae are. Abbott, the company which manufactures these Pediasure and Similac, reported that their profits increased by 55% or almost $200 million in 2013,
I was never a fan of Pediasure; its only advantage was that it was delivered by a medical supply company to our door. While it did not cost us any money now, I learned that we would probably have to pay about $7500 annually out of pocket for Pediasure once Margot turned 21, unless about 18 000 people ahead of her on the Pennsylvania Adult Waiver waiting list suddenly died.
And constipation?
So I became even less of a fan of Pediasure when I began to suspect that it might be contributing to chronic, severe, and uncomfortable constipation. We tried various solutions (prune juice, Miralax, Pediasure with fiber), with intermittent success. I began to wonder whether there might be a way to introduce certain high-fiber foods into her MIC-KEY button. A meeting with a nutritionist affiliated with Margot's primary care confirmed that this was possible.
Can I create a blend of foods to replace Pediasure?
I began with a simple meal of cooked oatmeal. I blended it with Pediasure so that it would be thin enough to pass through her tube. Since this has become her first meal each day, she is now rarely constipated. So I began to wonder about shifting her off of Pediasure entirely. Margot's nutritionist suggested a variety of foods that I could considering incorporating, that were healthy and rich in fibers or calories (One of these was black bean soup. A hint: don't make black bean soup the first real food you try with someone with a long history of constipation).
But Margot's nutritionist did not know of an existing resource that listed all of the kinds of foods that would work, or the amounts that might make for a healthy diet. And nothing turned up in my extensive google searches. So I was on my own to start to create specific recipes that might together constitute a more complete and balanced diet. What kinds of foods do I include? How much? How do I grind them up? It was challenging because the food had to be thin enough to pass through her tube, yet still carry the requisite calories. Over a period of several months, I developed a number of recipes that contained different foods that could be pureed. These all use foods that were reasonably calorie rich but not extraordinarily difficult to prepare in quantity.
It took me about a year to transition her to a diet consisting of about 70% real food, and 30% Pediasure (which we will eliminate entirely once we verify she can tolerate the increase in volume). Margot is no longer constipated, she is the right weight for her height for the first time in her life, and she began her menstrual cycle. And now, two years later, we have begun the final step to transition her off of Pediasure entirely.
In the greatest of ironies, Margot's disability may make her one of the healthiest adolescents in the county. She has the potential for the optimal diet, with the right balance of fruits, vegetables, fat, and fiber. She eats butternut squash and kale we have grown in our garden, and fresh apples and pears from a local orchard. She has - and will never - eat fast food or drink soda.
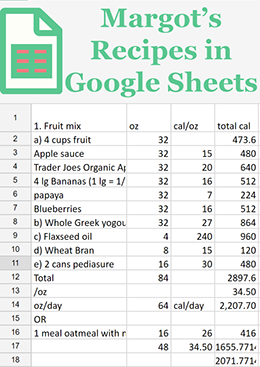
You can read more here about how I worked to find the right food, the right amounts, and the right equipment. The most recent recipes replace Pediasure and different dairy-based calorie-rich products with soy- and rice milk while maintaining a relatively high calorie count (abut 25 calories/oz of liquid). These new recipes also yield giant concentrated cubes that you freeze in advance for easier transport (essential to planning longer trips where access to a grinder and blender might be difficult), and that you thaw by adding soy- and rice milk to achieve the right amount of liquid and calories. And you can access the Google Sheet I developed to track Margot's calories and adjust her diet so that she was receiving a balanced diet of 2000 calories per day. You are welcome to give it a try (with guidance from your doctor, of course!).
Other Related Content

Margot's Recipes

About Margot
Born in 2000, Margot went straight into the NICU for a month
GoPro Hero
Everyday, incredible
accomplishments captured on video
Smile!
3 providers, 4 months, 5 appointments, too many phone calls, to fix 1 cavity
Real food, real meals
From drip-feeding a chemical blend to real food. Recipes included!
No "Can't Do"
A new video challenging assumptions about what Margot can enjoy and do.
Siege or surrender
On a Christmas trip to the tropics, I waved a white flag to our new reality.
Prisoner of Routine
Creating functional & fun routines took lots of effort but salvaged our sanity.
Trail Adventures
A blog for the Rails to Trails Conservancy offers tips to help hit the trails.
Leap of faith: Act I
My hopes took a hit, so I needed inspiration to take risks again, like kayaking.
Leap of faith: Act II
Inspired to kayak? From idea to implementation, and a lesson for research.
It's all downhill!
Can Margot learn to ski? With expert help and sensible teaching, yes!
Best summer ever!
After 18 years, getting summer right for Margot and the whole family!
The logo is adapted from Joaquim Alves Gaspar's drawing of Pedro Reinel's compass rose.
Connect