Making prevalence relevant, again
Using data from the ADDM network to help close gaps in implementation
No research about ASD has reliably garnered reaction from the professional and parent community like updates to estimates of ASD’s prevalence provided by the Centers for Disease Control or the CDC. According to the most recent report provided by the CDC, ASD occurs in 1 out of 68 individuals or in 1.5% of the population. When the CDC released its first report in 2007, ASD's prevalence was estimated at 1 in 150 individuals, or 0.7% of the population.
Initial reports of increased prevalence fueled concerns about an ASD "epidemic", and helped to mobilize a national research and policy agenda that became the 2007 Combating Autism Act. Each subsequent report has also sparked important discussions: Are we confident that these prevalence estimates are accurate? If so, is the number of people with ASD actually increasing, or are we simply getting better at detecting it? If ASD is actually increasing, what might be causing this?
A broad consensus has emerged among researchers, that these apparent increases do not reflect a burgeoning epidemic sparked by unknown causes. Instead, these apparent increases are more likely to reflect improved recognition of a spectrum condition that can sometimes take more complex or subtle forms. In the meantime, clear causes for ASD remain elusive, making it less likely that prevalence research will shed much light on the origins of ASD. Given this consensus, is research on prevalence still as relevant to addressing the challenges of ASD? The answer is yes, IF we can shift the focus to addressing the growing need for services. Otherwise, prevalence research risks becoming increasingly irrelevant.
Why is this shift needed? A second look at these reports reveals that many children with ASD continue to be diagnosed very late, or may not be diagnosed at all. In fact, since these gaps first became apparent almost 10 years ago, we seem to have made relatively little progress towards closing them. Even though the CDC's Learn the Signs Act Early national campaign has successfully mobilized teams in many different states, there appears to be no coordinated plan to systematically and rigorously test the range of possible strategies. Until we close these gaps, children with ASD cannot quickly or easily access the effective interventions we have begun to identify.
In this series of opinion pieces, I take a second look at the kinds of gaps revealed by the CDC's reports. By re-framing data from these reports, and combining these data with information from other sources, patterns emerge that may offer insights into the possible reasons for these gaps, and that suggest strategies for closing them. These patterns and associated strategies could help us pivot towards implementation of a coordinated program of research and policy. Such a program could systematically test how we develop and deliver effective programs to identify ASD in a broad and diverse population, and provide immediate and important benefits to people living with ASD.
The fact that such a program does not already exist, after two decades of public concern and intense research into the apparent increase in ASD's prevalence, is itself interesting. Does this reflect the limitations of our predominant model of science and public health, which emphasizes treatments derived directly from a cause, for a distinct disease identified in a population of individuals? What if ASD is not a disease that a person must be cured of? What if ASD is a characteristic that varies from one person to another, and that must be considered when choosing interventions for co-occurring conditions? In this case, we may need to count the likelihood that our services result in satisfactory and healthy outcomes, instead of counting the number of individuals who are diseased. Could this new perspective help to re-align our public health initiatives related to ASD?
Click on any description to read more.
Questions we can ask
What we may learn
Some background
 Estimates of ASD's prevalence reveal that many children may not be properly identified with ASD, let alone benefit from specialized services. This widening gap should concern advocates, researchers, policy makers, and program leaders alike.
Estimates of ASD's prevalence reveal that many children may not be properly identified with ASD, let alone benefit from specialized services. This widening gap should concern advocates, researchers, policy makers, and program leaders alike.
How do you estimate the prevalence of ASD?
 Estimating how many people have a rare and complex condition is a difficult task. The CDC's approach to select and evaluate a sample of children has raised important questions. Do these yield estimates that are reliable enough to begin to build on?
Estimating how many people have a rare and complex condition is a difficult task. The CDC's approach to select and evaluate a sample of children has raised important questions. Do these yield estimates that are reliable enough to begin to build on?
Are these methods accurate enough?
 Tests of the accuracy of the CDC's approach suggest that we may still be under-estimating ASD. These also reveal that the signs of ASD can be completely missed or just misinterpreted. And that some children with ASD may not be getting any help at all.
Tests of the accuracy of the CDC's approach suggest that we may still be under-estimating ASD. These also reveal that the signs of ASD can be completely missed or just misinterpreted. And that some children with ASD may not be getting any help at all.
Missing ASD has great consequences. Developing programs to catch it takes time, but must be prioritized
These data can help generate hypotheses about trends in identification without knowing ASD's true prevalence
Some children with ASD are completely missed.
Others may receive other services, but signs of ASD are being missed or misinterpreted.
In some states, the system of care, and the professionals driving it, may miss ASD in the majority of cases
Who is to blame for missing ASD?
 Do professionals need more training in screening and diagnosis? Maybe, but barriers connecting children to specialized assessment and inter- vention can create dis-incentives. Do they miss fewer children when we break these barriers?
Do professionals need more training in screening and diagnosis? Maybe, but barriers connecting children to specialized assessment and inter- vention can create dis-incentives. Do they miss fewer children when we break these barriers?
How do we miss an ASD diagnosis?
 Is prevalence so high because we completely miss ASD in so many children? In some cases, yes, but CDC data suggests other possibilities: ASD can be diagnosed later, mis-diagnosed, or viewed as secondary to other problems. Each tells a different story about ASD's complex nature.
Is prevalence so high because we completely miss ASD in so many children? In some cases, yes, but CDC data suggests other possibilities: ASD can be diagnosed later, mis-diagnosed, or viewed as secondary to other problems. Each tells a different story about ASD's complex nature.
Are some groups more likely to be missed?
 CDC data suggest that some groups, like traditionally under-served children and those without intellectual disabilities, are more often missed. Each gap reveals something different about how we can help more children with ASD.
CDC data suggest that some groups, like traditionally under-served children and those without intellectual disabilities, are more often missed. Each gap reveals something different about how we can help more children with ASD.
How many are we completely missing?
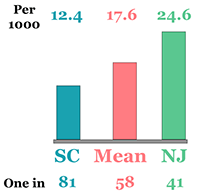 Is ASD more prevalent in some regions? Probably not, though sometimes more children are missed than are detected. And the number of children missed and the types of gaps probably vary greatly from state to state?
Is ASD more prevalent in some regions? Probably not, though sometimes more children are missed than are detected. And the number of children missed and the types of gaps probably vary greatly from state to state?
What is ASD's "true" prevalence?
 Labeling a child with ASD matters if it helps connect them to specialized supports. Prevalence matters if it helps scale up the support network. So can we know ASD's "true" prevalence if we cannot begin to deliver what children really need?
Labeling a child with ASD matters if it helps connect them to specialized supports. Prevalence matters if it helps scale up the support network. So can we know ASD's "true" prevalence if we cannot begin to deliver what children really need?
Coming soon
The logo is adapted from Joaquim Alves Gaspar's drawing of Pedro Reinel's compass rose.
Connect