Train & Hope??
![]() Training is necessary but often insufficient to ensure adoption of new practices.
Training is necessary but often insufficient to ensure adoption of new practices.
White elephant
![]() Create effective, sustainable programs before sinking money into a new building.
Create effective, sustainable programs before sinking money into a new building.
Implement, baby, implement
![]() Is traditional autism research becoming a bridge to nowhere?
Is traditional autism research becoming a bridge to nowhere?
Research to guide services
AutismSpectrumNewsNot all research is equally relevant to those focused on providing services.
A Network on Excellence
 Can statewide training increase expertise and capacity, and bridge gaps?
Can statewide training increase expertise and capacity, and bridge gaps?
A Bus to Betsy's
 The nominee to lead special education in the US could send it back to the Stone Age.
The nominee to lead special education in the US could send it back to the Stone Age.
The Business of innovation
 New services are shaped not by research but by available funds, staff, and expertise.
New services are shaped not by research but by available funds, staff, and expertise.
Margot votes! Will others?
 Learn how people like Margot exercise their right to vote in the 11 states that allow it .
Learn how people like Margot exercise their right to vote in the 11 states that allow it .
CoVid's silver lining
 Insights into the isolation and costs of disability might finally spur policy changes.
Insights into the isolation and costs of disability might finally spur policy changes.
A State of Synchro
The magic of teaching someone like Margot to ski mobilizes a remarkable army.
A Drop in the Bucket
New data suggests ASD research has little impact on improving identification.
The Delaware Network for Excellence in Autism
Can a new statewide training initiative increase expertise and capacity while bridging important gaps between sectors?
January 31, 2017
A new training program being launched in Delaware offers interesting lessons in what may be possible with strategic and coordinated advocacy across different sectors. It also reveals some of the pitfalls that await.
A quick summary
The Delaware Network for Excellence in Autism or DNEA grew from seeds planted by a statewide task force convened by the Center for Disabilities Studies and involving a wide range of stakeholders. CDS is the University Center on Excellence in Developmental Disabilities or UCEDD located at the University of Delaware. The resulting strategic plan, the Blueprint for Collective Action was published in July 2013. To follow up recommendations from the Blueprint related to public education, a separate Education Task Force was created through legislation passed in June 2014. I acted as a consultant to this Task Force. This Task Force developed two bills to define the DNEA, formally mandate a statewide inter-agency committee (the Inter-Agency Committee on Autism, or ICA) that had been recommended in the Blueprint, and other related changes to state code to provide the needed support for both the DNEA and the ICA. One of the two bills - Senate Bill 93 - providing basic support for the DNEA and ICA was passed in June 2016.
With respect to the DNEA, the Act is intended to "provide a resource for training and technical assistance for Delaware state agencies, organizations and other private entities operating in the State of Delaware who provide services and support to individuals and families affected by ASD". The bill includes funding to support a Director, four team leaders, and two Family Navigators. The DNEA is operated through a contract established with CDS (with a subcontract with Autism Delaware for the Family Navigators), and is guided by the ICA.
An important caveat. The story I tell below sometimes references input I offered, because I cannot speak for the Task Force, nor can I presume that the network will function in the ways I imagined. In the final analysis, the contributions and commitment of all partners to the collaborative process was far more important to whatever success has been achieved. This particular group of leaders and advocates were determined to make something better for Delaware, regardless of whether it might benefit themselves or their agencies. And that kind of commitment is priceless!
Related Content
On this site
Why focus on training if you want to improve services?
In my 2013 review of statewide service and training programs, I focused on 5 possible elements that contribute to better outcomes for people living with ASD: services, training, research, policy, and advocacy. Services are pivotal in this model, The impact of training, research, policy, and advocacy on outcomes is mediated by programs of services that are readily accessed (see diagram below).
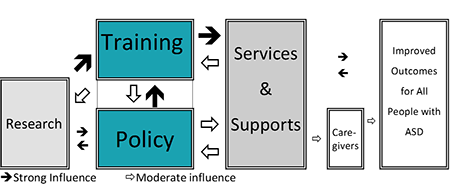 As part of this review, I also considered how four of these elements are funded, developed, and delivered. I also considered these in the light of the prevalence of the different types of needs to be addressed, and the intensity and degree of specialization required. This analysis suggested that statewide programs are best positioned to impact training and policy, while regional or local programs are best positioned to directly impact services and national programs are best positioned to guide and support research (see above diagram). These conclusions shaped my recommendations to the Task Force to focus on training and policy.
As part of this review, I also considered how four of these elements are funded, developed, and delivered. I also considered these in the light of the prevalence of the different types of needs to be addressed, and the intensity and degree of specialization required. This analysis suggested that statewide programs are best positioned to impact training and policy, while regional or local programs are best positioned to directly impact services and national programs are best positioned to guide and support research (see above diagram). These conclusions shaped my recommendations to the Task Force to focus on training and policy.
Why create a network?
When you are trying to improve outcomes without a huge investment of additional funds, one of the first things to look for is a service need that cuts across different agencies but that is falling between the cracks. The goal is to bundle resources from different agencies to create a bigger and better program than any individual agency might otherwise create. In my 2013 review, I identified several needs that cut across almost all sectors and agencies: ASD identification, support for challenging behaviors, case coordination for more complex children, and caregiver/self-advocate training, especially in accessing core services (more about these cross-cutting needs later).
This kind of cross-cutting need is perfectly suited for a well-coordinated network, but is a struggle for one agency to lead. Why? Housing a training initiative in one agency (like education) would put other agencies in the perceived position of deferring to another "expert" agency and funneling (often scarce) resources to another agency. This also makes it less likely that any agency other than the lead will feel true ownership. I recommended that the DNEA sit outside of state government - at University of Delaware - to avoid these specific pitfalls.
There are other considerations to housing a statewide training network at a university. On the plus side, universities are naturally suited to integrate training, policy, and research, especially those with a UCEDD (Doehring, 2013). It is important, however, to carefully assess a center's actual track record of community collaboration. While I consider CDS's record to be very good, I have found that other universities sometimes seem o be too busy touting their "unique expertise" to be a good partner with community agencies. The independence gained by housing a network outside of state government is another plus, though universities may be reluctant to jeopardize a lucrative contract by questioning a state mandate. A disadvantage is the hefty overhead (aka the indirect fees) levied by universities on grants, which can be as high as 40% if not negotiated beforehand.
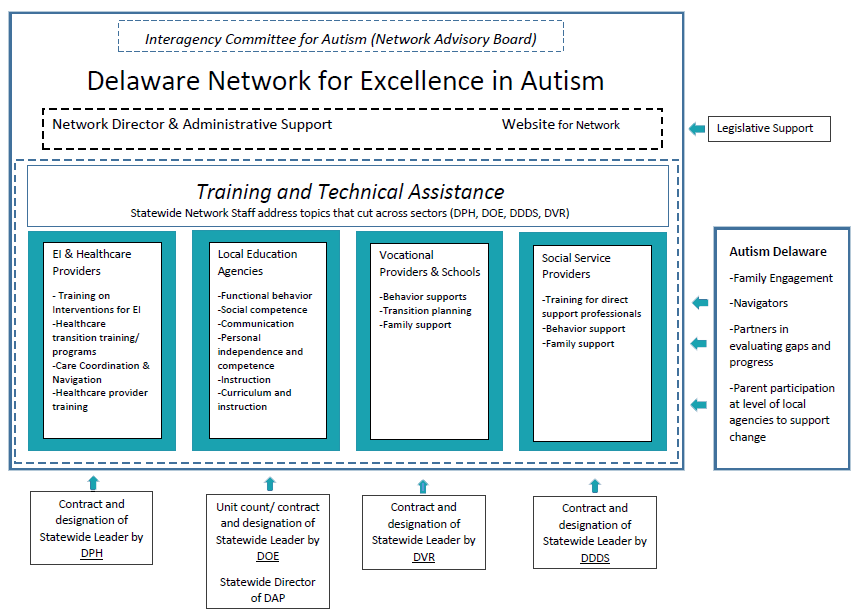
A well-structured network also has the potential to leverage resources from multiple sources. This is captured in a diagram of the network I presented at a meeting of the Task Force, largely adopted in the final draft (see below). For example, I anticipated that each partner agency would designate someone as a point person for the network, and who might assume leadership for matters relating to ASD within their on agency. This point person would parter with a designated DNEA Team Leader for specific training initiatives. Over time, this partnership may help to grow expertise and funnel policy and practice within each agency, to the collective benefit of the network.
I also envisioned that any funding and resources currently dedicated to addressing these cross-cutting needs within the agency might be re-directed to the network, to create a more powerful program of training when merged with other partners. And I was also excited to include a specific role for Delaware's primary advocacy group, Autism Delaware, in housing the Family Navigators. This leverages Autism Delaware's experience in - and longstanding commitment to - advocacy and policy (more about this below).
Where Statewide Initiatives have the greatest impact
What other lessons can be learned from statewide networks created elsewhere? Many different states have created networks, although my review (Doehring and Rozell, 2014) found that the kinds of training they undertook was highly variable, and often limited in scope. Too often, a "network" is a euphemism for an unfunded mandate; the DNEA has a clear funding stream with designated staffing. Some networks are really just committees that intend to act but never really do; the DNEA is legislatively mandated to provide training and support. The collaborative nature of networks can diffuse responsibility; the DNEA is designed to report to the ICA, and to report annually to the Governor and the Legislature. Each of these potential pitfalls was specifically addressed in language that I recommended be included in the legislation.
If the goal is to improve outcomes achieved through public schools, why not just focus on education?
The original impetus of the Task Force was to develop a more specific action plan to ensure better services in the schools, but shifted almost immediately to address a bigger opportunity. Why? The advantages of a network approach as listed above certainly provided a compelling argument, but there were other political considerations.
Like it or not, legislation is increasingly perceived as zero-sum game, especially when there is a fiscal impact in a conservative budget environment. If new resources are directed towards one sector, it appears to decrease the likelihood that another sector will also get new funding. Of course, we argued how better education programs would cut costs associated with consultation and private placement in more complex cases that could have been prevented had better services been available (and we included data on these costs). A network that aspires to have a broader impact renders the zero-sum argument irrelevant.
What about the immediate concerns for public education that sparked the creation of the Task Force? I also recommended that the DNEA begin by focusing on 2 to 3 cross-cutting needs of particular importance to the schools, and spend the first 1-2 years developing training primarily within the education system. This addresses a separate and significant practical problem, that we were unlikely to find off-the-shelf training packages we could readily implement. Developing a package first within the school system capitalized on the relatively greater concentration of services and expertise already available in the Delaware Autism Program. And there were many needs to choose from. In addition to the cross-cutting needs described earlier, there are other pressing needs that span education and at least one other sector: transition planning, employment, in-home parent support, and so on. Developing a complex program in phases also helps to maintain focus on specific goals and document progress for funders concerned about costs.
Other concerns surfaced about a focus on ASD to the exclusion of other disabilities. Again, a zero-sum scenario is often applied here: if more resources are devoted to helping children with ASD, it becomes less likely that other new resources might be designated for children with deafness, with other developmental disabilities, and so on. At various points during the development of this proposal, and even in discussions surrounding other legislation still to be passed, the benefits of an approach that included people with other kinds of disabilities was discussed.
Two options I proposed may be of interest to others facing this conundrum. First, some of these cross cutting needs are relevant to other populations. For example, many of the evidence-based practices for addressing challenging behaviors in children with ASD are just relevant to children with intellectual disabilities but without ASD. By beginning with needs that also cut across populations, we can help to diffuse the expertise through the initial workshops by including practitioners from other sectors in initial workshops, and making sure the content was not education specific.
Second, I proposed that we could always build into a 3-5 year plan a deadline for extending the trainings to other relevant populations. This addresses the practical problem described earlier: even had we had wanted to deliver a training relevant to multiple populations, we would likely need 2-3 years to develop a training for a specific sector and/or population before trying to generalize it. But we could certainly commit to extending training to other populations after this initial 3 year development phase. The most significant barrier to expansion lies in the more intensive individualized coaching and feedback that is often required. As discussed below, I had anticipated that this would be folded into the responsibilities of the experts we would cultivate within each agency.
Is there any way to provide direct and immediate support to people living the ASD?
One specific recommendation from the Blueprint was that Delaware consider developing a resource center to improve access to and utilization of services. The possible structure and role of a resource center was the focus on some of the Task Force's initial discussions. This discussion ranged from a physical to a virtual (e.g., web-based) center, and from a simple repository to something paired with a service that included some support to families.
I explored the potential of resource centers for other agencies, and included resource centers in the 2014 review of statewide initiatives. I do not believe that simply collecting information about resources and making it available to families has any enduring impact on outcomes. Using this information to help families navigate systems of care and access all available supports can, however, have an immediate and significant impact. I have described many examples of the barriers that families face in my 2013 review, in a detailed case description of a young man descending into a significant - but entirely preventable - behavioral crisis, and in the stories about trying to address my own daughter's dental and nutrition needs.
I was therefore excited to outline a potential role for Family Navigators in Delaware that would not only provide an important service but that would also gather important data for training and policy. I first outlined a role for Navigators as a follow-up to a successful grant submission for the Pennsylvania Act Early Team. The grant seeded a first phase centered on a Pennsylvania Autism Roadmap that paired an innovative on line resource directory with a sophisticated on line roadmap to accessing services (which became the CAR Autism Roadmap). In a second phase, I anticipated that staff from a range of agencies would not only be trained to field calls from families using the roadmap, but would gather information on the gaps and barriers that families faced. Information about these gaps and barriers would then be fed back to state agencies to help them set priorities for new programming.
The opportunities in Delaware were even greater. Pennsylvania does not have an active inter-agency autism committee: the information about the gaps and barriers faced by families and gathered by Delaware's Navigators in the course of their work could directly inform statewide planning undertaken by the ICA (I provided language to that effect in the legislation itself). This feedback would also inform the DNEA, by identifying what parents might be confused about, which could then inform the training that providers receive to better anticipate parent's questions. This addresses an important lesson I had learned earlier in Delaware: that advocates must be equal partners in helping to set priorities for programs.
I also recommended that Navigators be contracted through Autism Delaware, to take advantage of a pool of experienced parents. I was specifically interested in those parents compelled to stay at home because of their child's extraordinary needs. These parents are not only knowledgeable and motivated to help, but might jump at the kind of flexible, part-time work that the job of Navigator might offer.
Is the network coordinated with other state activities?
In my reviews, too many statewide initiatives stall because they do not build on - or may even conflict with - other related initiatives. It is not uncommon for a state education agency and a state behavioral health agency to each develop statewide training programs impacting mental or behavioral health. Or for a university to launch a new services initiative that is completely disconnected from the priorities established by a statewide committee. Or for a statewide committee to include no meaningful representation from a key sector, like public health or education.
I was excited to try to weave the DNEA and the ICA together. My reviews of statewide committees like the ICA had suggested had they are not suited to direct planning and oversight. I therefore recommended specific language in the legislation to reflect the complementary roles of the DNEA in training, and of the ICA in planning, policy, and monitoring. For example:
- Training was identified by the ICA as a principle means to improve outcomes, and so the DNEA becomes the implementation arm of the ICA (this is why the Director of the DNEA is a member of the ICA).
- Many training programs do not grow out of a coherent, long-term plan or benefit from the input of multiple stakeholders. The DNEA derived its priorities directly from the Blueprint.
- Many training programs do not change over time in response to evolving needs. I viewed the ICA as the monitoring and planning arm of the DNEA.
What pitfalls should we anticipate?
Let individual agencies fulfill their unique mandates, and focus on cross-cutting needs
The most common misconception about statewide training initiatives is that these somehow can or should address all of an agency's needs. Even in the publicity surrounding the passage of the legislation supporting the DNEA, I heard parents and agency leaders alike list a wide range of training that the DNEA would undertake. This is both unrealistic and unnecessary.
It is important to recognize that an initiative like the DNEA is best suited for training needs that bridge sectors (health, education, family/community-support, and so on) and agencies (like schools, hospitals, universities, and community-based agencies). As described in my 2013 review, these cross-cutting needs include ASD identification, support for challenging behaviors, case coordination for more complex children, and caregiver/self-advocate training in accessing core services. And there are other needs that bridge at least two sectors or agencies.
When agencies promote different- and sometimes competing - models of services, progress slows, resources are wasted, and families are confused. Training programs that bridge sectors can also help to align these models, when such alignment is possible and is appropriate. In the long-term, these might even support efforts towards more coordinated planning at the level of individual treatment or program development.
Interventions to address challenging behaviors are a case in point. Though the conditions that might be give rise to a problem behavior, and the types of interventions that might be prioritized, will vary between home and school, school- and community-based providers should use the same assessment approach and draw from the same evidence-based intervention toolbox. They will often end up identifying the same functions and developing similar plans. A coordinated training program also helps different providers speak the same language.
At the same time, there are training needs and training resources that are specific to sectors and to agencies that a cross-agency should never seek to address. Health and education programs each address needs that will rarely if never concern the other. And schools and hospitals have specific requirements for their staff to meet. Each state agency - and many local agencies - had designated experts for lead other kinds of training, and other people to support this training. A statewide training initiative like the DNEA should never substitute for, supplant, or usurp these efforts, but add to or enhance them.
Recognize that a statewide training initiative is just one piece in a larger training puzzle
Re-casting the individual agencies and sectors as pieces in a larger training puzzle may open our eyes to other pieces in this puzzle, and how a statewide training initiative might fit with them. For example, the training that professionals need for licensure offers some limited opportunities to increase knowledge about ASD: can a statewide initiative like the DNEA complement this? Advocacy organizations sometimes provide training to orient parents of newly-identified children to resources: can a statewide initiative complement that?
Two opportunities stand out for me. While statewide training initiatives like the DNEA can - and should - continue to bring in outside experts for specific topics, it will nonetheless be better positioned to fully utilize this expertise. Too many agencies rely on one-off workshops; the training topic de jour has everyone excited, a noted speaker is brought in, the speaker probably just gives the same talk he or she gives everywhere, everyone is energized and the agency appears progressive, and then absolutely nothing changes. This is similar to the popular but wholly unsuccessful Train and Hope approach of Program Development. In my 2013 book, I describe how to shift from one-time workshops to contracts that engage an expert in training, coaching, and feedback, as part of broader plan of program development. I find that experts thrive in this role, end up tailoring their training to met local needs, and become invested in having an impact.
Second, all agencies have leaders who may be competent managers but may not had expertise in ASD. And many agencies struggle to help individual professionals to grow into ASD experts who can help to lead new training initiatives - including those promoted in coordination with the DNEA. This is especially true for agencies that do not specialize in ASD, and small- to medium-sized agencies that lack the flexibility to carve out a new role for one of their professional staff. To expand competence or to increase capacity, you must cultivate new experts recruited within the organization. Any DNEA initiative that seeks to designate a point person within an agency to help implement hew practices, or builds on a train-the-trainer model, may help support the emergence of a new expert. And if you are lucky, you may also create a pipeline for new program leaders who also have content expertise.
Be cautious about investing heavily in a statewide conference
Autism advocates and funders eager for impact rush into building new facilities that become white elephants: the state conferences that statewide committee invest in can create something similar. To be fair, state conferences can serve a valuable function: they can disseminate specific initiatives, celebrate accomplishments and re-energize partners, bring in other experts to inform the work of the statewide committee, and provide an opportunity for the face-to-face contact needed in a long struggle. I had the chance to present at such a conference in Georgia in 2016.
But statewide conferences alone will never play a major role in truly advancing expertise or ensuring cross-agency collaboration: a smaller, invitation only annual meeting can accomplish more. And anyone who thinks that organizing a statewide conference open to the public is not incredibly difficult and resource intensive should host their own. There may be a place for an enhanced, invitation-only annual meeting - and sometimes even a public conference - but only if this constitutes a small piece of the total work undertaken by a statewide committee or training initiative.
Increase basic access to services
One way to have an immediate and significant impact, with no significant increase in funding to direct services, is to make sure that everyone knows how to quickly access services that are already available. This can involve online resources or in-person workshops (like the NextSteps workshops), especially if these are coordinated with community groups to reach traditionally under-served groups. Even better, we can provide families with real help in accessing services , and use the resulting feedback to improve services, as the DNEA's Family Navigators are intended to do. In either case, funders will always want to make sure people make best use of existing services before funding new ones.
But there are still other, perhaps more surprising opportunities. For example, these same resources can also help professionals who are themselves confused about other services, and how they might best refer families. Many professionals misunderstand the role of other professionals and agencies. Multidisciplinary training programs like LENDs can address this, but are relatively rare. And disciplines less likely to work in multidisciplinary teams (like behavior analysts) are at greater risk. I discovered that professionals were attending the NextSteps workshops originally designed for parents because they needed the same information. They were very positive about specific content I added to help parents understand what each discipline and each agency did after the initial diagnosis. That led us to pilot the first spin-off, the Next Steps for Professionals.
I am fascinated when the professionals who deliver these services also provide the orientation to families and other professionals trying to access them. As a facilitator of this process during the NextSteps workshops and elsewhere, I wait for that magical moment when a parent expresses confusion or frustration about accessing a service, and the professional either providing that service or a similar service has to respond. Professionals have remarkably few opportunities to experience this kind of accountability, and the best ones learn from it. I included this experience in the training of our LEND fellows to shape this kind of accountability from the start. When this occurs in the context of a training initiative that also informs statewide planning and policy, the stage may be set for real change. And to the extent that it starts with concerns from parent or front-line professional that are too often ignored, it fuels the kinds of empowerment needed for profound system change.
The devil in the details, especially in funding
People new to this type of work may want to heed lessons offered elsewhere on this sit, like the time and expertise needed to develop collaborative networks, or to embark on program development. But the most elusive piece of the puzzle is - no surprise - funding. The legislation passed in June 2016 - Senate Bill 93 - established the mandate and structure for the ICA and DNEA, and a base level of funding. A sister bill - Senate Bill 92 - sought to fund approximately 15 "Training Specialists" to support the training of educational professionals and parents, under the guidance of the Statewide Director of the Delaware Autism Program. This bill was not passed in June 2016, but efforts are underway to re-introduce it.
No one disputed the potential contribution of these Training Specialists. They are intended to supplement the 4 Team Leaders already funded through the DNEA. They can provide additional training and, more importantly, the hands-on coaching and support needed translate training into practice. These specialists would be funded using the same formula are the majority of educators in Delaware: about 60-65% of state funding, and about 35-40% local (e.g., property tax) funding - what heretofore I will refer to as local costs. And these specialists would dramatically increase the reach of training, and decrease the need for schools to send students to specialized centers outside of their district. But state and local costs are major drivers of decision making in Delaware (and indeed in most other states), and increased costs are one major reason this bill stalled.
But I suspect that one devilish detail also played a major role, and offers an important lesson to other states. Like many other states, Delaware's school districts are slow to create specialized public school programs or services that cross district boundaries. To be sure, most states have some kind of arrangement whereby a student in one district may attend a specialized program in another district. In these cases, the student's home school district pays some kind of "tuition" to the district housing the specialized program, to cover the local costs of delivering education (the state costs would typically be covered no matter which district the student attends). This is an efficient way to bundle programs too specialized to be easily delivered in every single district, or to cover the cost of specialized county-level school programs like those operated by the Delaware Autism Program.
But it gets more complicated when the public school district program only seeks training or consultation. We could imagine a specialized training program in one district that simply bills the school district receiving the training or consultation. This would be an efficient way to provide other specific supports that are too specialized for any one school district to easily develop on their own. But this occurs far less often than you think. To obtain other specialized services, schools find it more convenient to either ship a student to a program outside of the district, or to hire a an expert from outside of the public school system. The price of this convenience? We may unnecessarily perpetuate specialized and separate centers instead of educating children in the school closest to their home, or we pay for specialized private schools, or we pay to develop expertise that sits in private agencies outside of the public school system.
Delaware has been paying the price of this convenience for some time. School districts operating sites of the Delaware Autism Program benefit from training, monitoring, and other service programs operated by the Statewide Director, but usually without paying any of the local costs. The local costs have just been absorbed by the district that hosts the statewide program. This district does not want to create a separate tuition charge for these services, and then bill other districts for it. Why? Perhaps because of the additional work, or because of the blowback from other districts happy to receive specialized support for free. But the result is that specialized statewide services cannot grow unless the host district wants to absorb even more costs, even though the number of students with ASD continues to grow by 5-10% each year, even though more districts are eager for specialized training, and even though districts together send a least a million dollar each year out of the state for specialized training that could be provided within - and help to grow - a public school system.
Am I unnecessarily obsessed by this detail? Maybe, but this kind of inflexibility in how specialized public school services are delivered and funded is the greatest barrier to building our capacity to support students with more complex needs. Public schools in the United States have the potential to develop incredible expertise, if they can share resources. Instead, we have thousands of school districts across the country, each determined to go it alone, until legal action or behavioral crisis compels it to pay extraordinary costs for a private school or residential placement that is entirely avoidable. Delaware's problem is all too common.
Train & Hope??
![]() Training is necessary but often insufficient to ensure adoption of new practices.
Training is necessary but often insufficient to ensure adoption of new practices.
White elephant
![]() Create effective, sustainable programs before sinking money into a new building.
Create effective, sustainable programs before sinking money into a new building.
Implement, baby, implement
![]() Is traditional autism research becoming a bridge to nowhere?
Is traditional autism research becoming a bridge to nowhere?
Research to guide services
AutismSpectrumNewsNot all research is equally relevant to those focused on providing services.
A Network on Excellence
Can statewide training increase expertise and capacity, and bridge gaps?
A Bus to Betsy's
The nominee to lead special education in the US could send it back to the Stone Age.
The Business of innovation
New services are shaped not by research but by available funds, staff, and expertise.
Margot votes! Will others?
Learn how people like Margot exercise their right to vote in the 11 states that allow it .
CoVid's silver lining
Insights into the isolation and costs of disability might finally spur policy changes.
A State of Synchro
The magic of teaching someone like Margot to ski mobilizes a remarkable army.
A Drop in the Bucket
New data suggests ASD research has little impact on improving identification.
The logo is adapted from Joaquim Alves Gaspar's drawing of Pedro Reinel's compass rose.
Connect
X
My Related Publications

 (2014). Translating Research into Effective Social Policy. In Volkmar, F. Paul, R., Rogers, S., & Pelphrey, K. Handbook of Autism and Pervasive Developmental Disorders: Assessment, Interventions, Policy, the Future (4th ed.). John Wiley & Sons, Inc., Hoboken, New Jersey
(2014). Translating Research into Effective Social Policy. In Volkmar, F. Paul, R., Rogers, S., & Pelphrey, K. Handbook of Autism and Pervasive Developmental Disorders: Assessment, Interventions, Policy, the Future (4th ed.). John Wiley & Sons, Inc., Hoboken, New Jersey
 (2016). With Dena Gassner and Dan Crimmins. State of the Union, Keynote Conversation. Autism Conference & Exposition of Georgia, Center for Disability and Leaderships, School of Public Health, Georgia State University, Atlanta, GA.
(2016). With Dena Gassner and Dan Crimmins. State of the Union, Keynote Conversation. Autism Conference & Exposition of Georgia, Center for Disability and Leaderships, School of Public Health, Georgia State University, Atlanta, GA.
 (2014) With Denise Rozell. Beyond the Drawing Board: How statewide planning can generate and sustain improvement. Invited Workshop, National Autism Leadership Summit, Columbus, OH
(2014) With Denise Rozell. Beyond the Drawing Board: How statewide planning can generate and sustain improvement. Invited Workshop, National Autism Leadership Summit, Columbus, OH
Guideposts
![]() Simple Steps Launching a complex program in phases helps to maintain focus on specific goals, and to document progress for funders.
Simple Steps Launching a complex program in phases helps to maintain focus on specific goals, and to document progress for funders.
![]() Simple Steps Advocates must help to decide which services should be prioritized for their own child and for the overall program.
Simple Steps Advocates must help to decide which services should be prioritized for their own child and for the overall program.
![]() Other Lessons Improving and expanding services in a coordinated and sustainable way requires planning, expertise, and leadership
Other Lessons Improving and expanding services in a coordinated and sustainable way requires planning, expertise, and leadership
![]() Other Lessons There is no natural pipeline of leaders trained and experienced in undertaking comprehensive program development
Other Lessons There is no natural pipeline of leaders trained and experienced in undertaking comprehensive program development
![]() Other Lessons To expand competence or to increase capacity, you must cultivate new experts recruited within the organization
Other Lessons To expand competence or to increase capacity, you must cultivate new experts recruited within the organization
![]() Other Lessons Collaborative networks multiply the impact of new initiatives when they carefully draw on the strengths of each partner
Other Lessons Collaborative networks multiply the impact of new initiatives when they carefully draw on the strengths of each partner